PRP vs. PRF: What's the Difference?
Both start with your own blood — but activation changes everything. Here's how Platelet-Rich Plasma and Platelet-Rich Fibrin differ, and when each is used.

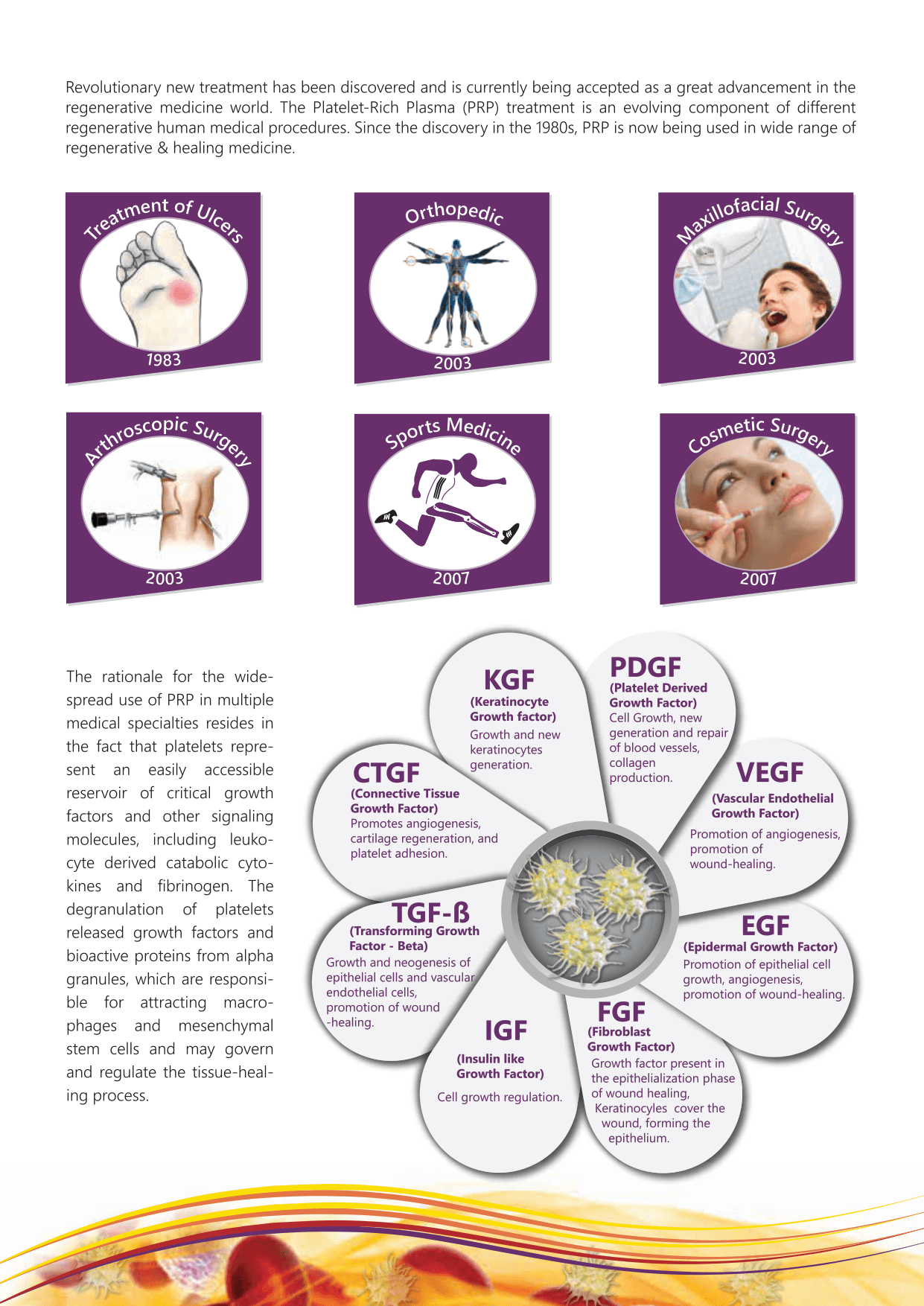
Platelet-Rich Plasma (PRP) is produced by centrifuging a patient's blood to concentrate platelets — the cells that carry the growth factors responsible for tissue repair. In this state the platelets remain inactive, and once injected they may migrate away from the target site.
Platelet-Rich Fibrin (PRF) is what you get when an activator such as calcium chloride is added to PRP. Fibrin threads begin to appear as a matrix, the platelets become activated, and that fibrin net holds them firmly in place at the injection site. The practical result: growth factors are released gradually, exactly where they are needed, over a longer period of time.
Prizmah is designed for both. Its closed system produces pure PRP without RBC and WBC contamination, and its built-in calcium chloride activation converts PRP into PRF gel within about 10 minutes — or a membrane within a minute using the PRF tray.
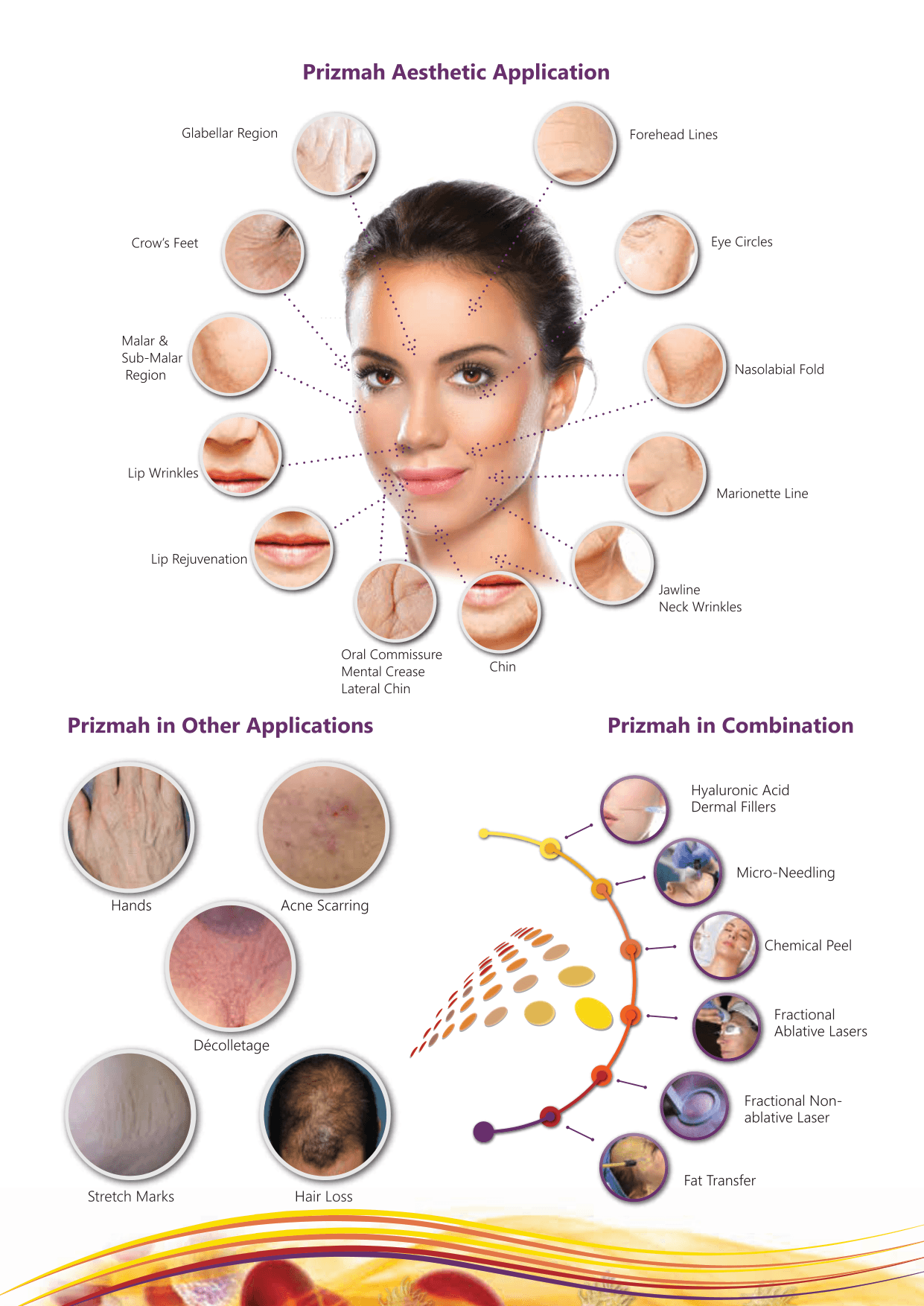
Which is right for a given case depends on the indication. Liquid PRP suits many aesthetic and orthopedic injections; PRF gel and membrane are especially valued in dentistry and wound management, where a scaffold that stays put and releases factors slowly accelerates soft-tissue and bone healing.
This article is derived from the official Prizmah clinical brochures and FAQ. It is for informational purposes and is not a substitute for professional medical advice.